





-
我国肝癌发病率占所有肿瘤疾病的第4位,病死率占第2位[1]。HBV或HCV感染、肝硬化等与肝癌的发病密切相关[2]。肝癌起病隐匿,进展迅速,多数患者临床症状明显或发现时已为中晚期,容易错失最佳手术时机。针对无法手术切除的肝癌患者,经肝动脉化疗栓塞术(transcatheter arterial chemoembolization,TACE)目前被公认为非手术治疗肝癌的最常用方法之一[3]。
TACE采用栓塞剂栓塞肿瘤动脉同时结合抗肿瘤药物,使肿瘤组织缺血缺氧并产生细胞毒性作用,从而诱导肿瘤细胞坏死[4-5]。但TACE术后不良反应发生率高,严重时甚至死亡。栓塞后综合征(postembolization syndrome,PES)是最常见的并发症[6],其病理机制为:当肝段动脉栓塞后,栓塞区域组织成片坏死、水肿;PES患者临床表现为发热、腹痛、恶心、呕吐、黄疸等。现代医学对此常采用的治疗方法主要为退热、止呕、止痛和保肝等对症治疗,但部分患者症状缓解欠佳;而中医药毒副作用较少,价格低廉,患者接受度高,能预防PES发生和缓解临床症状,提高介入治疗疗效[7]。中西医结合治疗可发挥各自优势,可更好地促进TACE术后快速康复,降低并发症的发生率,提高疗效。因此,本研究通过数据挖掘技术对临床中药用药进行数据分析,并总结临床用药规律,挖掘核心处方,以便更好地指导临床用药,为中医药治疗PES提供科学依据。
-
以《中国知网数据库》(中国知网)、《中国学术期刊数据库》(万方)、《中文科技期刊数据库》(维普)作为数据来源,采用“中药”、“TACE术后”、“栓塞综合征”、“TACE术后栓塞综合征”为关键词进行检索,时间范围是2000年1月至2021年12月,共检索到156篇期刊文献。
-
剔除综述类、实验研究类、组方重复出现、无具体药物组成或单味中药等文献,选择中药复方或中药制剂治疗的临床研究,最终筛选出符合标准的期刊文献84篇,方剂86首。
-
通过查阅《中华人民共和国药典》(2020年版)[8]和《中药学》(第3版)[9],将药物名称、分类、性味归经等进行规范处理,对具有不同名称的中药统一命名,如“生晒参”统一为“人参”,“玄胡”、“元胡”统一为“延胡索”,“八月札”统一为“预知子”等。
-
首先将上述中药逐一输入至Excel 2019,根据编号、方名、药名、类别、性味、归经等建立中药数据信息表;再对纳入的全部中药进行筛选排序,并使用SPSS Statistics 21.0和SPSS Modeler 18.0进行关联规则分析、因子分析和聚类分析等统计学处理。
-
86首方剂中含181味中药,累积频数942次;频率≥10%(药物频数/处方数)的高频中药共28种,累积频数587次。对频率≥10%的中药进行统计,其中,使用频数最高的前3位分别是甘草(53次,61.63%)、茯苓(51次,59.30%)和白术(45次,52.33%),见表1。
药物 频数 频率(%) 药物 频数 频率(%) 甘草 53 61.63 枳壳 15 17.44 茯苓 51 59.30 莪术 14 16.28 白术 45 52.33 山药 13 15.12 柴胡 39 45.35 生姜 13 15.12 黄芪 34 39.53 茵陈 13 15.12 白芍 30 34.88 太子参 11 12.79 半夏 30 34.88 薏苡仁 11 12.79 党参 28 32.56 栀子 11 12.79 当归 23 26.74 鳖甲 10 11.63 白花蛇舌草 22 25.58 赤芍 10 11.63 黄芩 20 23.26 人参 10 11.63 陈皮 18 20.93 延胡索 10 11.63 半枝莲 17 19.77 郁金 10 11.63 丹参 17 19.77 大枣 9 10.47 -
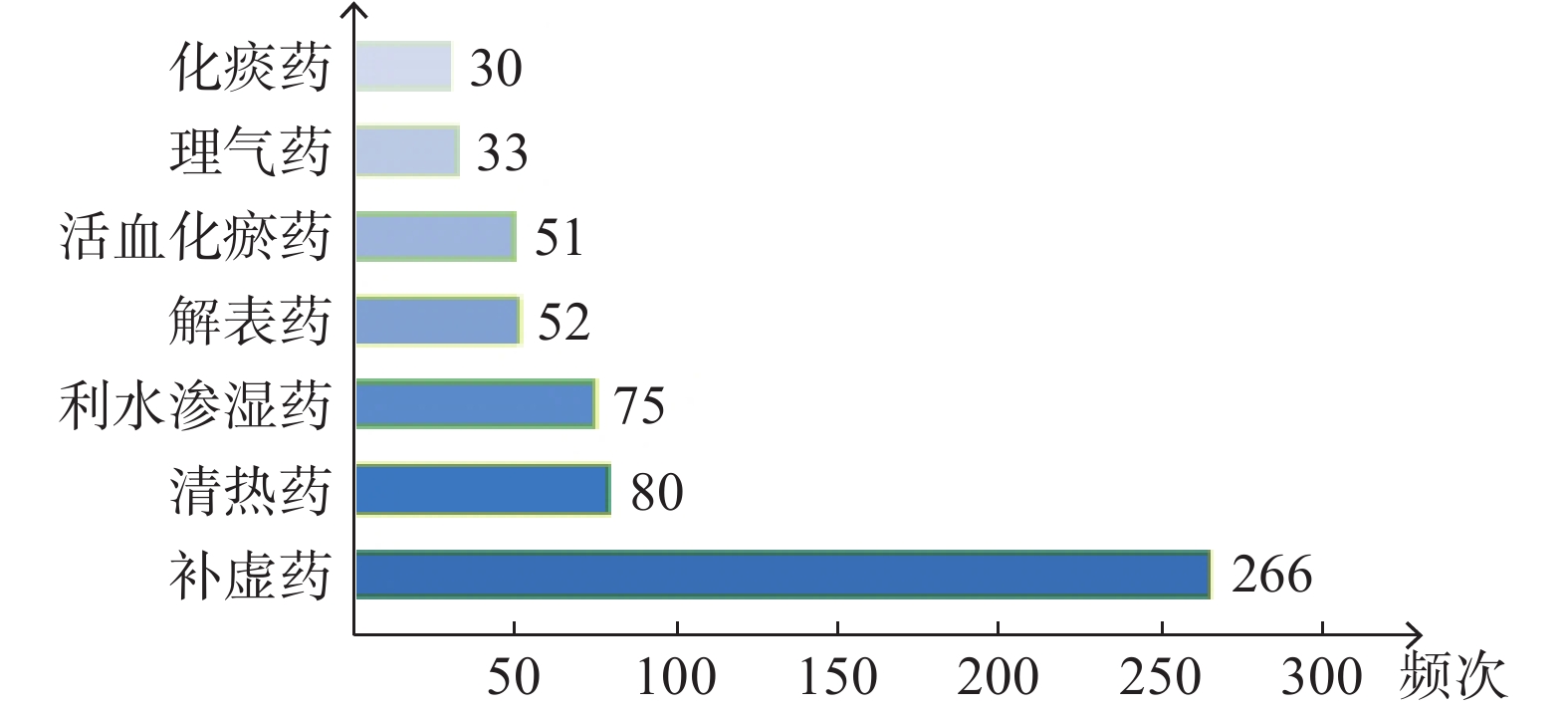
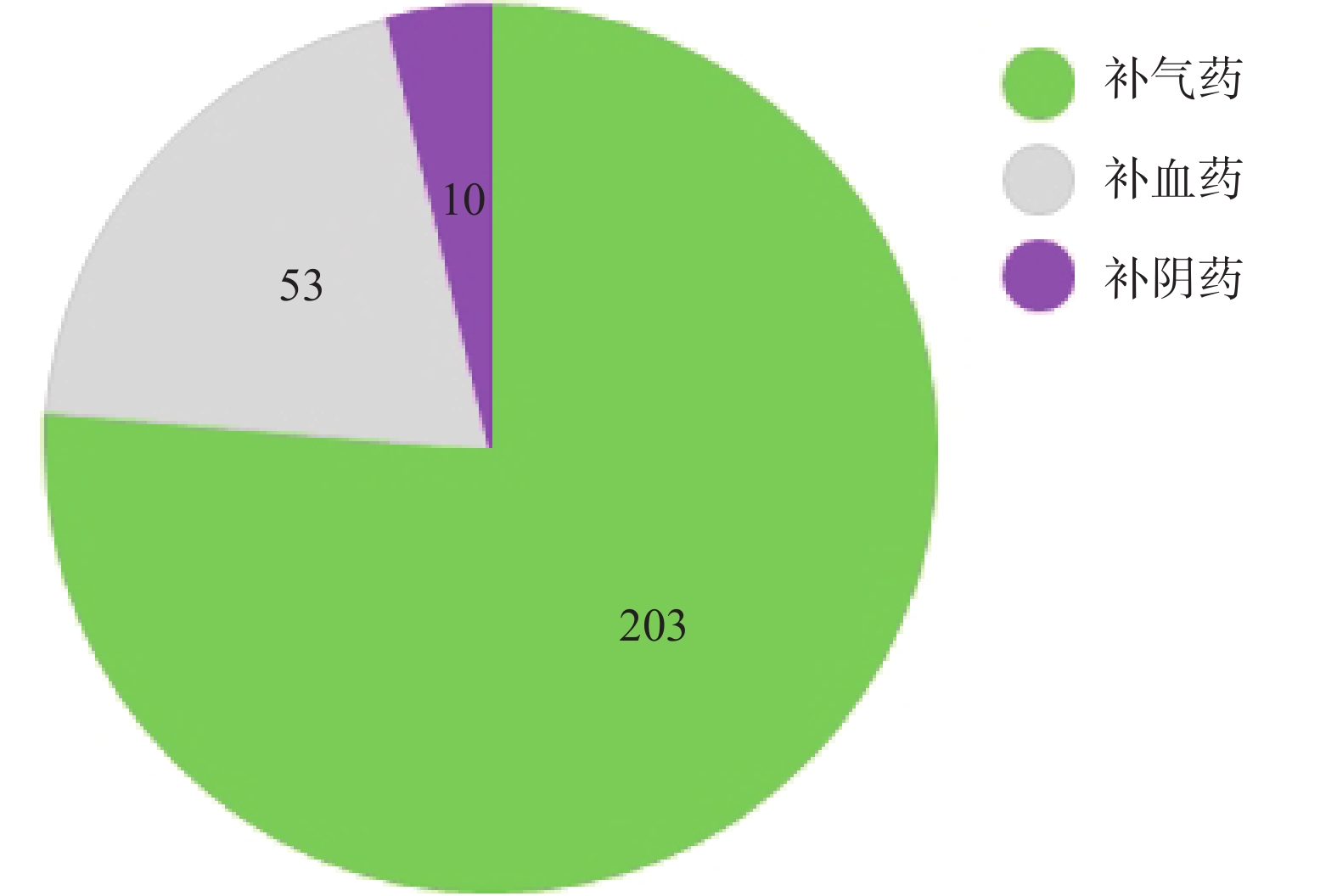
对频率≥10%的高频中药进行分类归纳,共包括7类中药。前3类中药分别是:补虚药(266次,45.32%)、清热药(80次,13.63%)、利水渗湿药(75次,12.78%),见图1。再根据气血阴阳的不同,对补虚药进行统计,从高到低依次为补气药(203次,76.32%)、补血药(53次,19.92%)、补阴药(10次,3.76%),见图2。
-
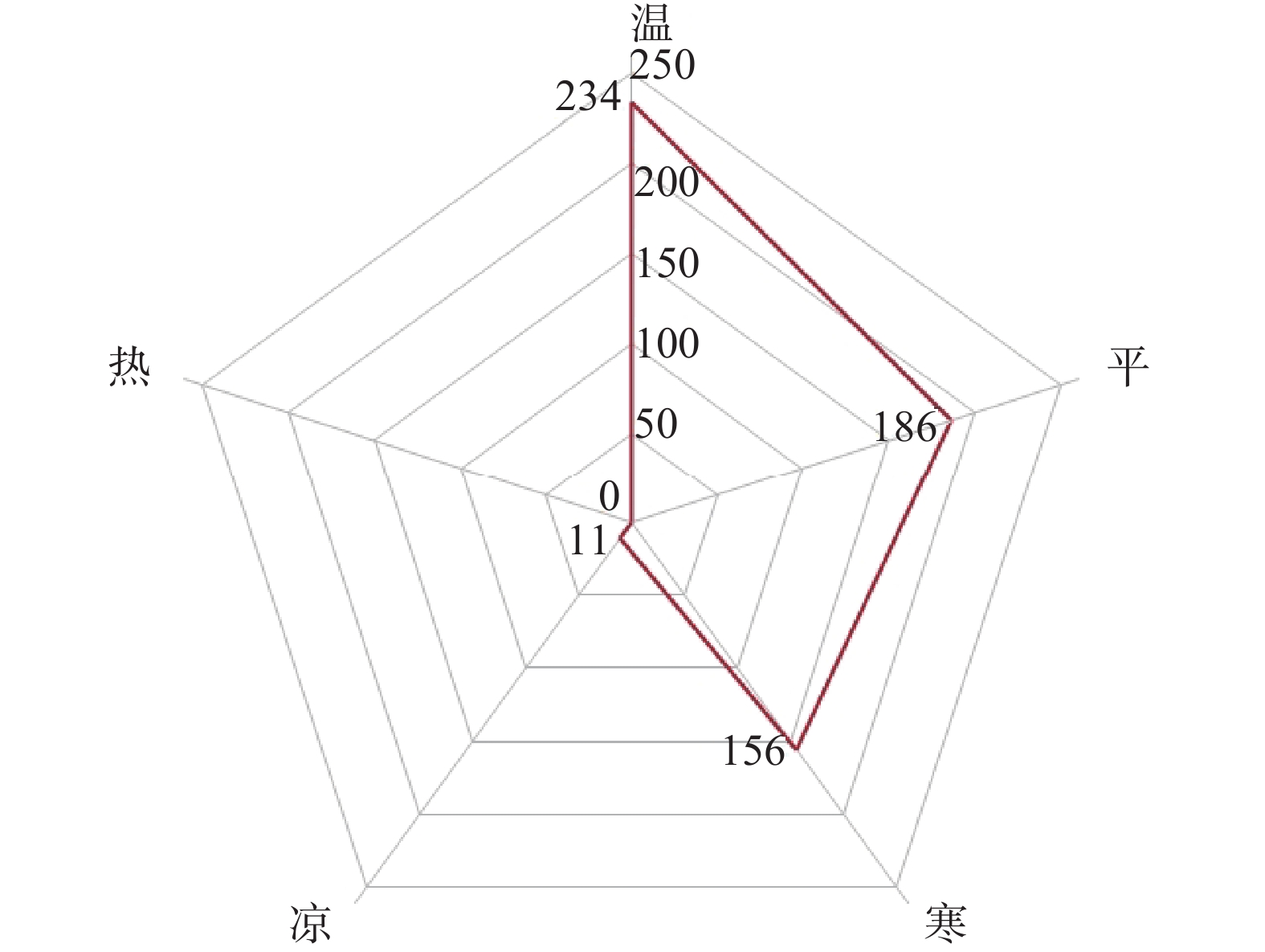
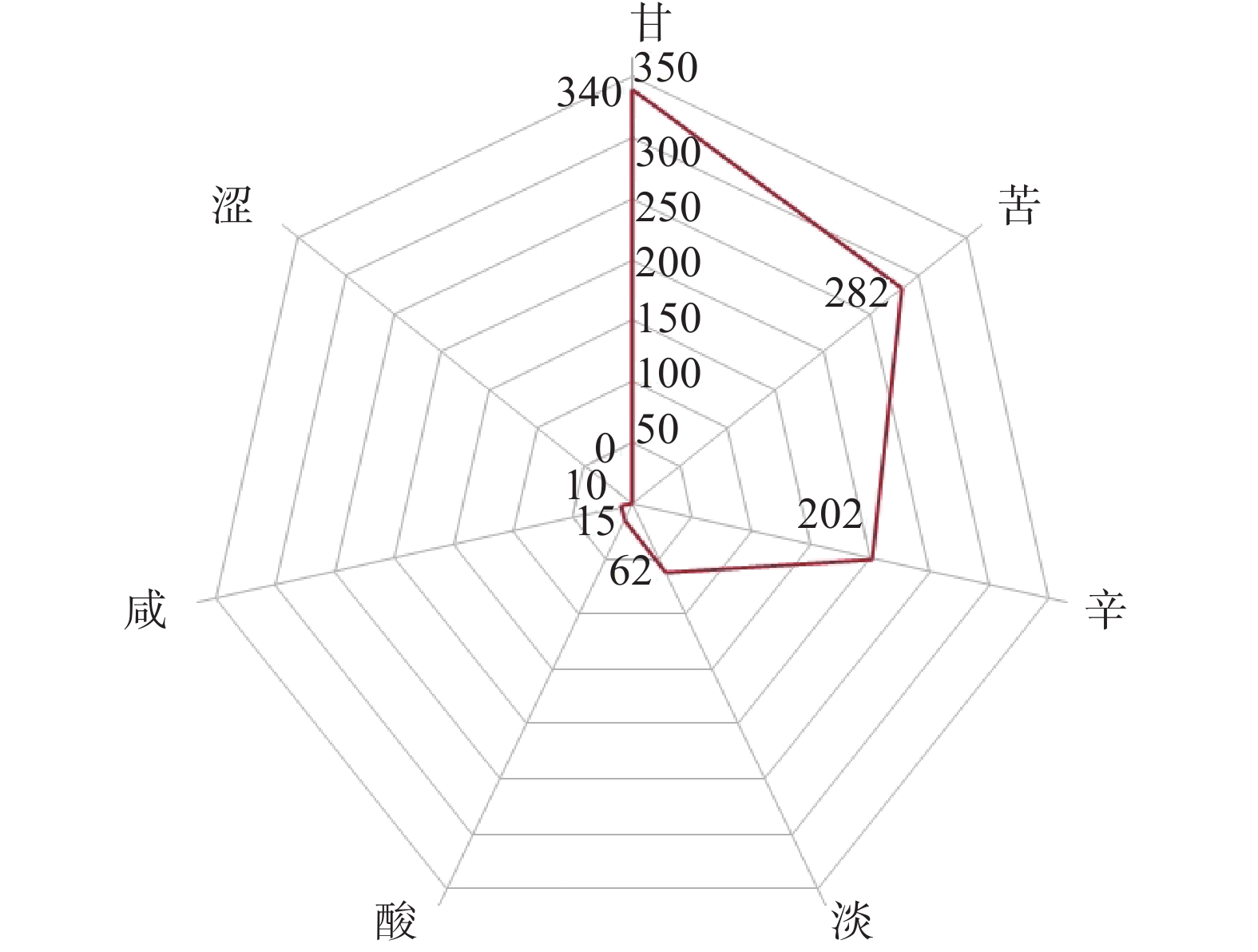
对高频药物(频率≥10%)的药性药味进行统计,结果显示,药性频数共计587次,药味频数共计911次。在药性分布中,前3类中药药性分别是:温(12种,234次,39.86%)、平(6种,186次,31.69%)、寒(9种,156次,26.58%),共占98.13%,见图3。在药味分布中,前3类中药药味分别是:甘(13种,340次,37.32%)、苦(16种,282次,30.95%)、辛(11种,202次,22.17%),共占90.45%,见图4。
-
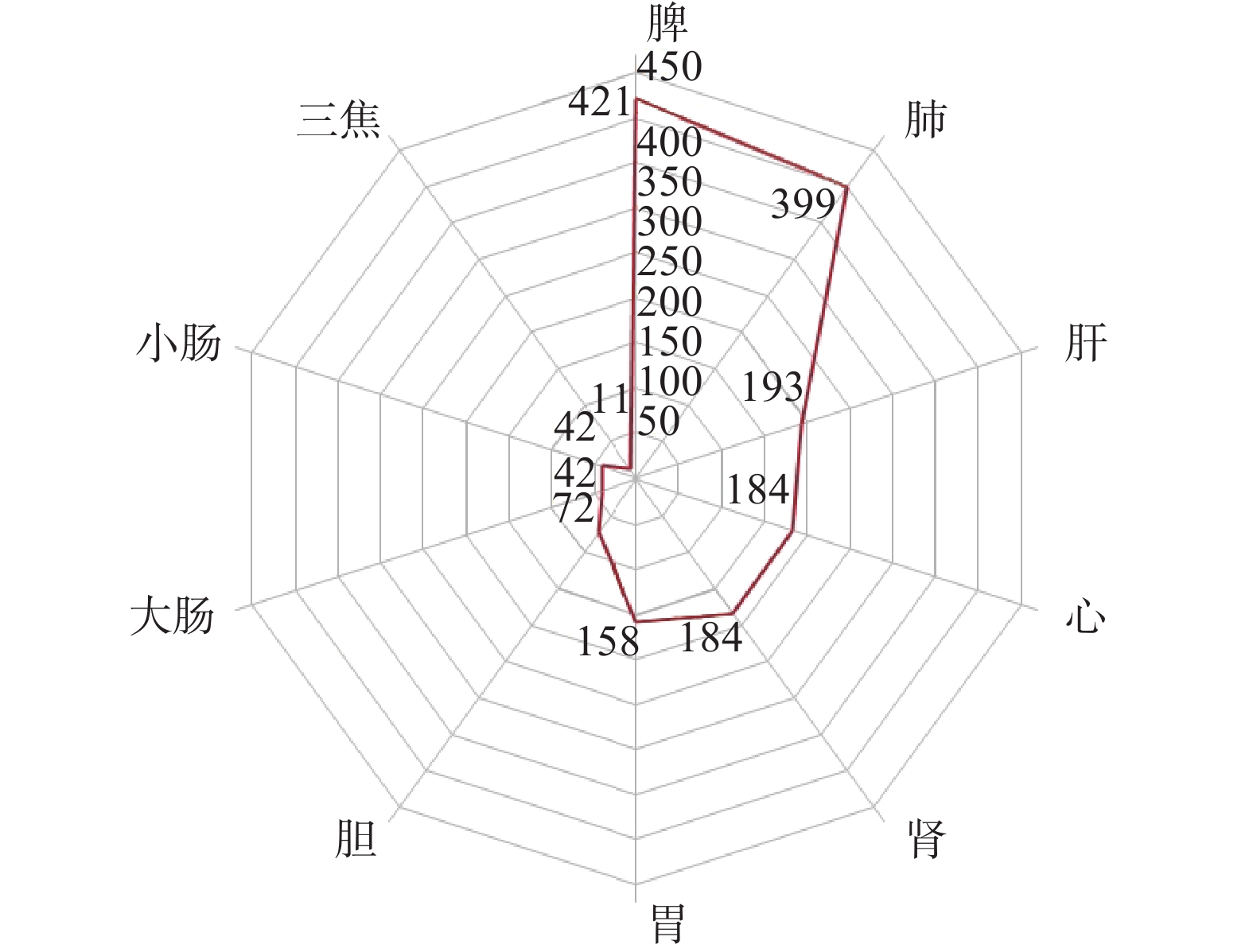
对高频药物(频率≥10%)的归经进行统计,结果显示,28味中药归经频数共计1 706次,其中,前3类中药归经分别是脾经(421次,24.68%)、肺经(399次,23.39%)、肝经(193次,11.31%),见图5。
-
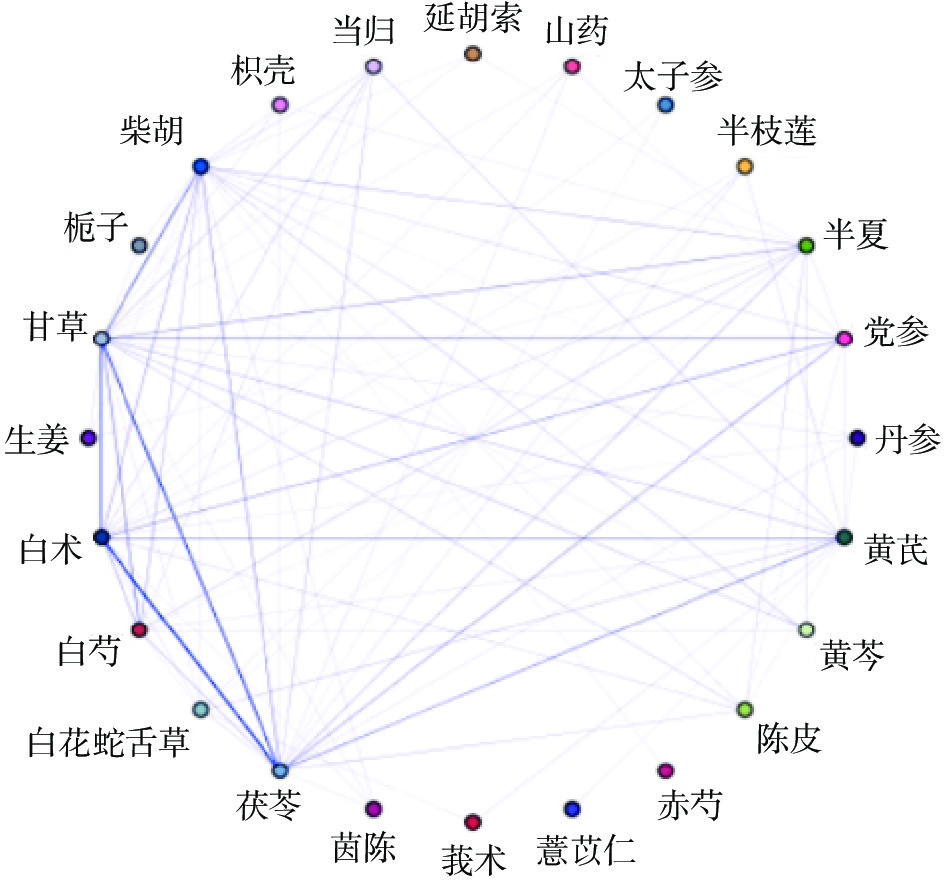
运用SPSS Modeler 18.0统计软件,对高频药物(频率≥10%)进行关联规则分析。先建立“源→类型→网络”数据流,得到药物规则分析网络,见图6;再通过Apriori建模进一步发现中药之间的联系,设置支持度为10%,置信度为100%,最大前项数为5,提升度≥1,删去重复组合,共得到30条关联规则,支持度前5的依次是:茯苓→党参和白术、茯苓→黄芪和白术、茯苓→党参、白术和甘草、茯苓→黄芪、白术和甘草、茯苓→陈皮和白术,见表2。
药物组合 支持度(%) 药物组合 支持度(%) 茯苓→党参和白术 26.74 茯苓→陈皮、白术和甘草 11.63 茯苓→黄芪和白术 26.74 白术→当归、白芍和茯苓 11.63 茯苓→党参、白术和甘草 19.77 甘草→当归、白芍和茯苓 11.63 茯苓→黄芪、白术和甘草 18.60 白术→党参、黄芪和甘草 11.63 茯苓→陈皮和白术 15.12 茯苓→党参、黄芪和甘草 11.63 甘草→黄芩、半夏和柴胡 15.12 茯苓→党参、柴胡和白术 11.63 白术→党参和黄芪 13.95 茯苓→半夏、白术和甘草 11.63 茯苓→党参和黄芪 13.95 茯苓→黄芪、柴胡和白术 11.63 茯苓→党参、黄芪和白术 13.95 甘草→当归、白芍、白术和茯苓 11.63 茯苓→白花蛇舌草和白术 12.79 茯苓→党参、黄芪、白术和甘草 11.63 甘草→当归、白芍和白术 12.79 甘草→生姜和柴胡 10.47 甘草→栀子和柴胡 11.63 茯苓→半枝莲、黄芪和白术 10.47 柴胡→茵陈和甘草 11.63 茯苓→陈皮、半夏和白术 10.47 茯苓→半枝莲和白术 11.63 白术→白芍、半夏和茯苓 10.47 茯苓→丹参和白术 11.63 茯苓→白芍、黄芪和白术 10.47 -
运用SPSS Statistics 21.0统计软件,对高频药物(频率≥10%)进行因子分析。统计前完成KMO和Bartlett的球形度检验,KMO值为0.556>0.5,Bartlett的球形度检验的χ2值为697.379(自由度为378),P<0.001,说明差异显著,数据具有较好的线性关系,适合做因子分析。通过旋转成分矩阵,得到11个公因子,累积方差贡献率71.716%,见表3。
公因子 中药 因子贡献率(%) F1 白术、茯苓、党参 13.545 F2 半枝莲、白花蛇舌草、黄芪、莪术 9.790 F3 茵陈、栀子、柴胡、黄芩 8.347 F4 陈皮、半夏、延胡索 7.066 F5 大枣、生姜 6.111 F6 山药、白芍 5.549 F7 太子参 5.126 F8 人参 4.817 F9 丹参、薏苡仁 3.976 F10 赤芍 3.755 F11 郁金、当归 3.634 -
运用SPSS Statistics 21.0统计软件,对高频药物(频率≥10%)进行聚类分析。选择组间连接,度量标准中的区间选择Pearson相关性,聚类选择为变量,得到聚类树状图,见图7。结合中药主治功效,将药物分为6类,聚类1:茯苓、白术、党参;聚类2:白花蛇舌草、莪术、黄芪、半枝莲;聚类3:丹参、鳖甲;聚类4:生姜、大枣;聚类5:甘草、白芍;聚类6:半夏、黄芩、延胡索、柴胡、栀子、茵陈。

-
中医学认为,肝癌患者早期气滞、血瘀、湿热等邪实相互搏结,日久成积,肝积即成,邪毒内蕴,耗气伤阴,导致气血亏虚,阴阳两虚,虚实夹杂、标本互见,成为本虚标实之证[10]。而TACE治疗,虽然是治疗措施,但也能成为致病因素,TACE治疗中化疗药物、栓塞剂等外来毒邪侵袭人体,进而使肝脾受到损伤,肝的气血运行不畅,脾的运化功能失常,机体气机壅滞、脉络阻滞,湿热聚集[11],从而出现以发热、腹痛、恶心、呕吐、黄疸等临床表现为主的PES,故中医治法应当以健脾益气,清热利湿,行气活血为主。
中药频次分析结果表明,治疗PES的用药包括补气药、清热药、利水渗湿药、补血药、解表药、活血化瘀药、理气药、化痰药;用药以补气药、清热药、利水渗湿药为最多,反映了PES本虚标实的病机特点,本虚以脾气虚为主,标实包括湿热、血瘀、气滞等实邪。
药物性味与归经分析发现,治疗PES的中药药性主要为温、平、寒;药味主要为甘、苦、辛。甘味可补益、和中、调和药性、缓急止痛,温性药能温中、散寒、助阳,甘温药如白术、黄芪可益气健脾;寒性药能清热泻火,苦味能泻火、燥湿,苦寒直折,苦寒药如黄芩可清热燥湿;辛味能散、能行,有行气、行血作用,《黄帝内经·素问》云:“肝欲散,急食辛以散之,用辛补之”,如柴胡味辛,可疏肝解郁。药物归经主要为脾、肺、肝经。PES虽病位在肝,但与脾胃密切相关,《金匮要略》有云:“见肝之病,知肝传脾,当先实脾”,故应当注意调理脾胃,防止肝病传脾,进一步加重病情。肝主升,肺主降,二者相互协调,调畅气机,当肝、肺失司,气机不畅,或会出现痰瘀互结,所以在治疗时还应注意疏肝调肺。
基于关联规则分析,在置信度为100%时,支持度前5的中药包括茯苓、党参、白术、黄芪、甘草和陈皮,这些药物与单味药用药频次统计结果具有高度的一致性,多为补气药,以四君子汤为基础。因子分析共得到11个公因子;聚类分析得到6个聚类,聚类1可健脾益气燥湿,聚类2清热利湿解毒,聚类3可养阴活血,聚类4可调和营卫,聚类5可缓急止痛,聚类6可清热退黄、利湿除满、和解少阳。综合关联规则分析、因子分析、聚类分析,可得到治疗PES的4个药物组合,分别是组合1:茯苓、白术、党参、黄芪、甘草;组合2:白花蛇舌草、半枝莲、莪术;组合3:柴胡、黄芩、半夏、生姜、大枣;组合4:茵陈、栀子。
组合1中党参功效似人参,可益肺补脾、养血生津,白术健脾益气、燥湿利水,茯苓利水渗湿、健脾补中,黄芪补气健脾、利水消肿,甘草益气和中,调和诸药,五药合用,共奏益气健脾祛湿之功效。白术、党参、茯苓、甘草4味中药在中医临床上常一起配伍成经典方剂——四君子汤。《时方歌括》曰:“胃气为生人之本,参、术、苓、草从容和缓,补中宫土气,达于上下四旁,而五脏六腑皆以受气,故一切虚证皆以此方为主”,四君子汤为古今益气健脾的基础方,以培土固本之法改善患者的正气不足之症,广泛应用于临床中。现代研究发现,四君子汤及其化裁方可有效提高免疫功能,调节肝功能指标[12-13],能抑制Hep G2肝癌细胞的增殖,诱导其凋亡[14],抑制H22荷瘤小鼠肿瘤生长[15-16],并抑制移植瘤血管新生[16]。
组合2中白花蛇舌草、半枝莲清热利湿解毒,莪术破血消癓、行气止痛,3药配伍,清热利湿、活血解毒。TACE治疗的患者大多为肝癌中晚期,虽行TACE术,但不能完全清除肿瘤细胞,邪气虽渐消,但仍有癌毒蛰伏体内,再者,TACE术后患者正气亏虚,易导致术后复发,治疗PES不仅要注重补益正气,还要注意抗肝癌中药的使用。现代研究发现,3药具有抗肝癌的作用,白花蛇舌草乙酸乙酯提取物可能通过抑制Nur77/JNK信号通路发挥抗肝癌作用[17],半枝莲多糖组分SBP-1A与SBP-2A对肝癌细胞Hep G2的增殖有抑制作用[18],白花蛇舌草与半枝莲提取物通过调控circRNA表达抑制肝癌细胞的生长[19],莪术中的β-榄香烯对Hep G2细胞具有明显的抑制作用[20]。
组合3是小柴胡汤的主要组成,组合中柴胡疏透郁邪,黄芩清泄火热,二者合用,和解少阳,解郁退热,如《本草汇言》曰:“清肌退热,柴胡最佳,然无黄芩不能凉肌达表”;黄芩苦寒,清热燥湿,半夏辛温,燥湿化痰,二者相合,辛开苦降,清热燥湿;《本经疏证》云,“《伤寒》《金匮》两书……姜与枣联,为和营卫之主剂,姜以主卫,枣以主营”,生姜温胃散寒,大枣补脾和胃,益气生津,二者配伍,可健运脾胃,调和营卫;生姜为“呕家圣药”,配伍半夏可降逆止呕;五药合用,和解少阳、清热燥湿、降逆止呕。有研究发现,小柴胡汤可有效地预防及治疗PES,在一定程度上缓解发热、呕吐、腹痛等临床症状,改善肝功能 [21-22],抗肝纤维化[23-24],促进Huh7细胞凋亡[25],增强顺铂对Hep G2肝癌细胞促凋亡效果[26], 抑制H22肝癌小鼠癌细胞的生长,并改善免疫水平[27]。
组合4中,茵陈清热利湿、利胆退黄,栀子,清热利湿、通利三焦,《本草通玄》有云:“仲景多用栀子茵陈,取其利小便而蠲湿热也”,二者配伍,引湿热下行,使湿热从小便出,从而清热利湿退黄。茵陈、栀子与大黄合为茵陈蒿汤,可清热利湿退黄,治疗湿热黄疸。有研究发现,鲜茵陈提取物及茵陈蒿汤能抑制Hep G2肝癌细胞增殖,促进细胞的凋亡[28-29],茵陈蒿汤可改善黄疸症状及指标[30],减少肝损伤,改善肝功能[31]。
综上所述,通过对中医治疗TACE术后栓塞综合征的临床研究文献归纳统计后,从用药频次统计以及统计学分析结果可知:临床用药以补虚药、清热药和利水渗湿药居多,治法以健脾益气、清热利湿解毒为主,而PES主要病机为正气亏虚、湿热聚集,数据挖掘结果与PES的病因病机及治则治法相符。本研究以中国知网、万方、维普数据库作为数据来源,筛选了中药治疗PES的临床用药文献,在一定程度上反映了临床治疗的整体用药趋势,可供临床医师在辨证论治的同时给予适当的参考,也为中药治疗PES深入研究奠定一定的基础。
Study on the regularity of traditional Chinese medicine in treatment of postembolization syndrome after TACE based on data mining
doi: 10.12206/j.issn.2097-2024.202208101
- Received Date: 2022-08-24
- Rev Recd Date: 2023-02-27
- Available Online: 2023-12-22
- Publish Date: 2023-12-25
-
Key words:
- liver cancer /
- transcatheter arterial chemoembolization /
- postembolization syndrome /
- traditional Chinese medicine /
- data mining
Abstract:
| Citation: | ZHONG Zhipeng, GUO Bingjie, XIAO Chulan, YIN Zifei, LI Bai. Study on the regularity of traditional Chinese medicine in treatment of postembolization syndrome after TACE based on data mining[J]. Journal of Pharmaceutical Practice and Service, 2023, 41(12): 747-752, 759. doi: 10.12206/j.issn.2097-2024.202208101

|
 DownLoad:
DownLoad: