


-
马兜铃酸(AAs)是存在于马兜铃科植物中结构相似的硝基菲羧酸类化合物,广泛存在于马兜铃属和细辛属植物中。含AAs成分的中药,如青木香、关木通、细辛、马兜铃等都有明确的肾毒性[1-2]。马兜铃酸肾病(AAN)是因服用含有AAs成分的药物而造成的急、慢性肾小管间质疾病,表现为肾小管变性、萎缩、坏死和广泛的肾间质纤维化[3],临床上以夜尿增多、贫血、消化道症状、高血压就诊者居多,易被漏诊和误诊。AAN急性肾损害患者大部分预后良好,慢性肾损害患者预后较差。笔者所在单位是全军肾病中西医结合治疗中心,每年均收治一定数量的AAN患者,但尚未进行全面的回顾性分析。本文就此开展研究,旨在分析AAN临床特点和规律,避免误诊漏诊,提高临床确诊率。
-
依据2004—2022年该中心收治的因服用含有AAs引起药品不良反应(ADR)报表中患者信息,对患者病历进行回顾性调查。
-
采用Excel 2007进行数据统计调查,内容包括患者性别、年龄、引起AAN临床表现、引起AAN药品、引起AAN药品服用时间、原患疾病、实验室检查等。计量描述以(
$ \bar{x}\pm s $ )表示,计数以频数(构成比/%)表示。 -
拟定评判ADR标准为:①明确有口服AAs成分药物史,临床诊断以间质性肾炎为主要诊断的AAN;②无长期或近期使用引起间质性肾损害的药物史,如解热镇痛药、抗菌药物、利尿剂等;③可排除临床系统性疾病伴发的肾小管间质病变、肾小球疾病、感染相关性间质性肾炎、肾动脉狭窄、高血压肾病及糖尿病肾病等;④典型病理形态学为寡细胞性肾间质纤维化及肾小管萎缩。最终确定AAN患者111例。
-
111例AAN患者中,男性31例,女性80例,女性多于男性(2.58∶1)。年龄最小者31岁,最大者 88岁,平均年龄(63.70 ± 11.67)岁,大于50岁的101例(90.99%),详见表1。
性别 年龄(岁) 合计 30~39 40~49 50~59 60~69 70~79 80~89 男 1 1 5 4 13 7 31 女 2 6 28 28 13 3 80 合计 3 7 33 32 26 10 111 构成比(%) 2.70 6.31 29.73 28.83 23.42 9.01 100.00 -
111例AAN患者中,服用AAs成分药物时间最长的30年,最短20 d,平均服药时间(8.08±6.94)年。107例(96.40%)服用超过1年,其中1~5年病例数最多,超过5年次之,10年以上的累计占36.04%,详见表2。
序号 服用时间(年) 数量(例) 构成比(%) 1 <1.0 4 3.60 2 1.0~<5 41 36.94 3 ≥5.0~<10 26 23.42 4 ≥10.0~<15 21 18.92 5 ≥15~<20 8 7.21 6 ≥20 11 9.91 合计 111 100.00 -
111例AAN患者中,服用冠心苏合丸和龙胆泻肝丸共106例(95.50%)。111例患者按药品说明书规定剂量服用62例(55.86%),随意服用45例(40.54%),不详4例(3.60%),111例中单用药103例(92.79%)、联合用药8例(7.21%), 详见表3。
序号 药物名称 例数 构成比(%) 原患疾病 1 冠心苏合丸 78 70.27 冠心病(38)、心前区不适(9)、风湿性心脏病(1)、急性心肌梗死(1)、间断胸闷+气短(1)、
口干+心慌(1)、心动过速(1)、心功能Ⅲ级(1)、心慌+气短(1)、心脏病(1)、不详(23)2 龙胆泻肝丸 22 19.82 祛火(7)、身体不适(5)、乙肝(3)、护肝(1)、酒后去肝火(1)、口腔溃疡(1)、
皮肤过敏(1)、眼干(1)、子宫肌瘤(1)、清肝明目(1)3 冠心苏合丸+龙胆泻肝丸 6 5.41 冠心病(3)、不详(3) 4 木通(中药饮片) 2 1.80 心前区不适(1)、不详(1) 5 耳聋丸 1 0.90 内耳眩晕症(1) 6 冠心苏合丸+冠心泰丸 1 0.90 不详(1) 7 龙胆泻肝丸+蛇王贝毒胶囊 1 0.90 不详(1) 合计 111 100.00 -
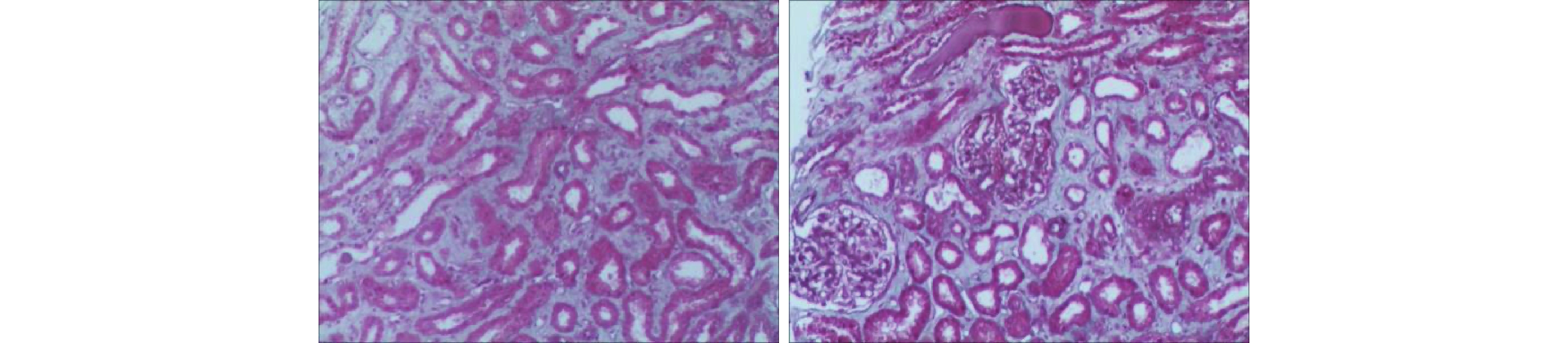
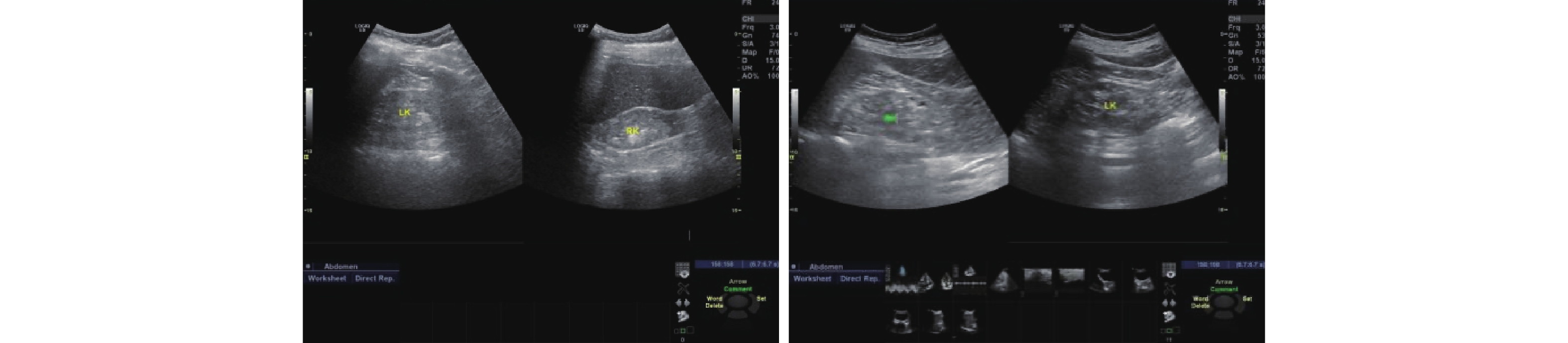
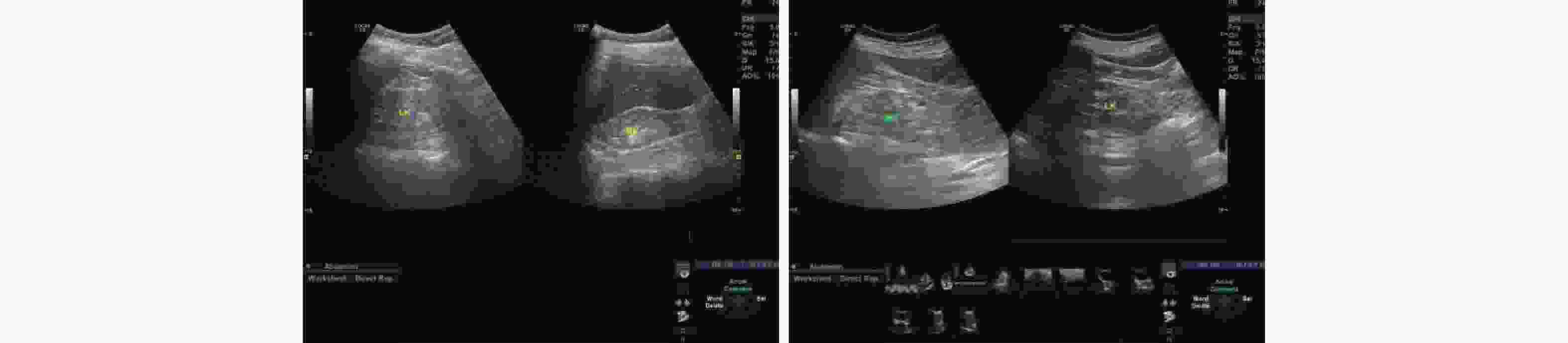
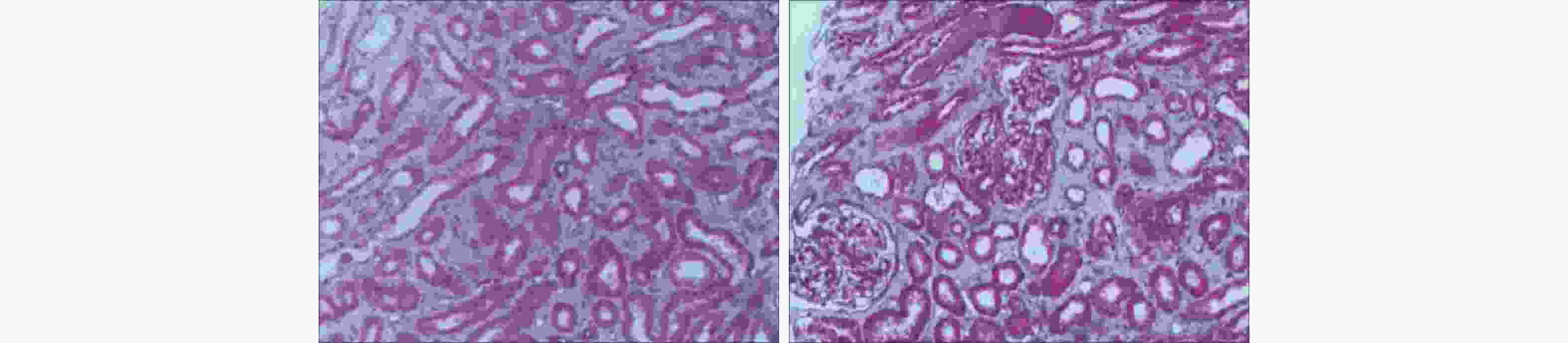
111例AAN患者中,实验室检查:血肌酐升高108例,结果范围为83~1600 μmol/L(514.31±206.48 μmol/L);尿素氮升高106例,结果范围为3.01~65.79 mmol/L(20.23±8.96 mmol/L);血红蛋白降低103例,结果范围为40~168 g/L(84.89±15.56 g/L),无检查结果7例;24 h尿蛋白区间0.1~4.1 g/d(0.48±0.35 g/d),多数为低比重尿,蛋白尿及潜血(±)~(+++)不等。超声检查肾脏均不同程度受损,呈肾体积缩小(大小不对称)、结构不清晰、弥漫性改变、血流不丰富等,详见图1。肾病理形态学多为肾小管上皮细胞脱落变性、肾小管萎缩,有不同程度的肾小管间质损害,典型的为寡细胞性肾间质纤维化,详见图2。多数患者起病隐匿,进展程度不一,与年龄、服药时间不成正比。临床上肾功能呈进行性损害,多数不可逆、预后较差,多表现纳差、夜尿增多,乏力、面色苍白、水肿不明显,多伴有贫血,贫血程度与肾功能减退程度不平行。临床均以AAN或因服用AAs药物引起的间质性肾炎和伴有进行性肾功能减退等原因收住院治疗。
-
111例AAN患者中,女性多于男性(2.58∶1),与有关报道[4]基本相似,可能因男女解剖和生理上有一定区别,女性较男性更易受药物影响[5]。其次,可能与绝经后女性因体内雌激素水平下降,易患更年期综合征、心血管疾病等,使用冠心苏合丸、龙胆泻肝丸治疗上述疾病会引起AAN的机会增加有关。本研究AAN患者年龄大于50岁共101例,占比90.99%。有报道指出,50~90岁人肾小球滤过率可下降50%,65岁后肝血流量为青年人的40%~50%[6],中老年患者肝、肾功能的降低会影响药物代谢,使半衰期延长,导致药物在体内蓄积,增加患AAN的风险。最新研究证明,肾脏血流动力学的改变及肾小管上皮细胞损伤后重吸收功能的异常也是AAN的致病机制[7]。
-
111例AAN患者中,服用含AAs药物最长的30年,最短20 d,107例服用超过1年。有研究发现,关木通临床等倍剂量提取物用药持续3周,可明显引起肾损害,证明肾毒性马兜铃酸累积阈剂量与给药剂量具有相关性[8]。中药中的很多成分是小分子物质,肾功能减退时肾脏排泄减少,加重残存肾单位药物负荷,药物在体内蓄积造成肾损害[9]。本研究发现,发生AAN的原因可能与长时间、超剂量服用AAs药物有关,使AAs在肾脏最主要的蓄积场所产生蓄积效应[10],引起肾功能减退,进一步加重肾功能损伤。
-
111例AAN患者中,涉及药物有7个品种,冠心苏合丸和龙胆泻肝丸共106例(95.50%)。本研究调查发现,患者服用冠心苏合丸和龙胆泻肝丸多在90 年代中后期,当时两药成分中含有AAs植物青木香和关木通,长期或短期服用可引起AAN。原国家食品药品监督管理局因青木香和关木通能引起AAN,于2003年将处方中的关木通换为木通,2004年将青木香替换为土木香,有效制止了青木香、关木通制剂引起的肾损害[11]。冠心苏合丸常用于冠心病、心绞痛的临床治疗,功效是宽胸、理气、止痛,用于寒凝气滞、心脉不通所致的胸闷、心前区疼痛的症状。龙胆泻肝丸具有泻肝胆实火、清下焦湿热的功效,主治肝胆实火上炎所致的头痛、目赤、胁痛、耳鸣等,以及肝胆湿热下注所引起的外阴瘙痒、小便淋浊、妇女带下等症。本研究调查发现,患者对中药毒副作用普遍存在认知偏差,认为中药没有毒副作用或毒副作用较小,多数患者为自我药疗,服药较随意,存在滥用现象。提示中药制剂应在中医理论指导下辨证施治,不可盲目擅自服用,避免引起药源性损害。
-
本研究调查发现,患者服用AAs时间与肾功能受损情况不相关,服用时间的长短与个体差异有关,与年龄、服药时间不成正比。如78岁男性,服用冠心苏合丸2年,血肌酐1600 μmol /L,尿素氮43.8 mmol/L。81岁男性,服用冠心苏合丸30年,血肌酐721 μmol /L,血尿素氮25.9 mmol /L。61岁男性服用冠心苏合丸6年,血肌酐83 μmol /L,尿素氮6.7 mmol /L。55岁女性,服用含有木通中药汤剂20 d,血肌酐377 μmol /L,尿素氮17.2 mmol/L。AAN目前尚无特异性诊断标准,当服用含有AAs中草药制剂而出现无法解释的进行性发展相对较快的肾脏病时,需对AAN的可能性进行排查[10]。有研究显示,在早期肾小管损伤检测中,黄醇结合蛋白、β2微球蛋白、胱抑素C、尿-乙酰-β氨基葡萄糖苷酶等较血肌酐和尿素氮有一定检测优势[12-13]。提示临床对出现贫血、肾功能损害及肾脏大小改变等的患者,应追问其服药史,以求尽快确诊救治。
-
AAs是一种广泛存在的毒性物质[14],其引起肾损害毒性最大的是马兜铃酸Ⅰ[15-16]。文献通过对急性AAN患者随访1~7年,其中一半的患者因肾衰竭需要透析治疗,另外一半患者进展成4期慢性肾脏病,持续性损伤发展为终末期肾病[17]。AAN的特点是肾功能损害进展迅速,即便停止使用含AAs成分药物,病情依然进展[18]。目前尚无有效针对AAN的治疗方法[10]。有报道低剂量糖皮质激素可延缓AAs诱导的肾功能减退[19];前列腺素E1对AAs诱导的急性肾脏微血管损伤可能有一定的治疗作用[20];AAs诱导的慢性肾损伤通过同基因间充质干细胞移植有治疗肾间质纤维化的作用[21];此外中药大黄附子汤[22]、丹参酮I可减轻AAs诱导的肾损伤等。以上方法因缺乏长期研究及病例数较少,尚难以对AAN疗效作出客观性评价[23]。在本研究中,临床通过中西医结合药物治疗,中药治疗为行益气养血固肾、活血化瘀、和胃降逆、通腑泄浊等辨证治疗,如百令胶囊、肾衰宁片、尿毒清颗粒、肾康注射液、中药汤剂等保肾降氮治疗,丹参川芎嗪注射液、冠心宁注射液、舒血宁注射液等活血化瘀治疗,叶酸、铁剂、促红细胞生成素等纠正贫血,硝苯地平、缬沙坦等降压治疗,对达到尿毒症期的患者行血液透析治疗,多数患者病情好转或稳定出院。
-
多数AAN患者因纳差、夜尿增多、乏力等原因就诊,实验室检查后,多有不同程度的血尿肌酐、尿素氮升高等肾功能损害表现,临床初诊多诊断为慢性肾功能不全、血肌酐升高、肾功能衰竭等,易造成漏诊、误诊。分析原因:①AAN临床表现不典型,最初表现以纳差、乏力、夜尿增多为主,如果检查不全面,易造成误漏诊;②接诊医师对AAN的临床表现及发病特点认识不足,实验室检查血肌酐、尿素氮升高,就草率诊断为肾功能不全、肾功能衰竭、血肌酐升高等;③非专科医师对AAs毒副作用认识不够,接诊医师对AAN的病因、鉴别诊断要点不熟悉或忽视;④医生问诊时对患者服用药物询问不详细,忽略患者曾服用含有AAs的药物;⑤AAN多发生于50岁以上的中、老年人,以女性居多,存在个体差异,有肾脏实质性疾病的患者反应更为敏感[24],初诊中要重点关注特殊人群。
AAs可通过一种或者多种机制导致不同程度的肾损伤[7]。肾损失患者个体差异较大,与服用AAs药物时间长短、剂量不相关,且AAN进展迅速,即使停止使用含AAs药物后病情依然进展。因此,进一步加强药物警戒工作,防范含有AAs成分药物引起的严重肾功能损害具有重要意义。临床诊疗过程中应重视对AAN的诊断,掌握AAN临床特点和规律,在中医药理论指导下辨证施治,进行早期的诊断和有效的干预,有条件的可进行治疗药物监测(TDM),有助于尽快确诊救治,避免误诊漏诊,减少AAN的发生或延缓其发展。
Analysis of 111 cases of aristolochic acids nephropathy
doi: 10.12206/j.issn.2097-2024.202308066
- Received Date: 2023-08-31
- Rev Recd Date: 2023-10-16
- Available Online: 2024-01-19
- Publish Date: 2024-01-25
-
Key words:
- aristolochic acids /
- aristolochic acid nephropathy /
- interstitial nephritis /
- Guanxinsuhe pill /
- Longdanxiegan pill /
- pharmacovigilance
Abstract:
| Citation: | SHI Wenhui, WANG Yanmei, JIANG Li, LI Jun, LI Xiaomeng, HE Zhijun. Analysis of 111 cases of aristolochic acids nephropathy[J]. Journal of Pharmaceutical Practice and Service, 2024, 42(1): 38-42. doi: 10.12206/j.issn.2097-2024.202308066

|

 DownLoad:
DownLoad: