

 下载:
下载:

-
近年来,有研究证实胰高血糖素样多肽-1(GLP-1)受体激动剂和钠-葡萄糖共转运蛋白-2(SGLT-2)抑制剂对2型糖尿病患者具有心血管保护作用[1-12]。中华医学会糖尿病分会第二十四次全国学术会议发布了《中国糖尿病防治指南(2020版)》,指南建议确诊动脉粥样硬化性心血管疾病(ASCVD)或伴有ASCVD高危因素的2型糖尿病患者,不论其糖化血红蛋白(HbA1c)是否达标,只要没有禁忌证都应在二甲双胍的基础上加用具有ASCVD获益证据的GLP-1受体激动剂或SGLT-2抑制剂;合并心衰(HF)的2型糖尿病患者,不论其HbA1c是否达标,只要没有禁忌证都应在二甲双胍的基础上加用SGLT-2抑制剂[13]。根据大型心血管安全性试验的结果,具有ASCVD获益的SGLT-2抑制剂和GLP-1受体激动剂有:恩格列净、卡格列净、利拉鲁肽、索马鲁肽、度拉糖肽和阿必鲁肽,其他SGLT-2抑制剂和GLP-1受体激动剂是否具有ASCVD获益还需进一步研究;具有心衰获益的仅有SGLT-2抑制剂:恩格列净、卡格列净、达格列净和艾托格列净,GLP-1受体激动剂是否具有心衰获益还需进一步研究[14]。本研究基于现有的证据进行系统回顾和网络Meta分析(NMA),评价已上市的SGLT-2抑制剂和GLP-1受体激动剂对T2DM患者心血管保护作用的疗效差异,对其进行概率排序,形成推荐等级,为我国2型糖尿病临床治疗方案的选择提供循证依据。
-
检索Medline、Embase和Cochrane Library数据库,检索日期为建库至2020年7月18日。采用主题词结合自由词的方式制定检索策略。检索词包括“diabetes mellitus, type 2” “randomized controlled trial” “empagliflozin” “canagliflozin” “dapagliflozin” “ertugliflozin” “albiglutide” “dulaglutide” “exenatide” “liraglutide” “lixisenatide” “semaglutide” “oral se-maglutide”。
-
①随机对照试验;②年龄≥18岁,2型糖尿病患者;③试验组:恩格列净、卡格列净、达格列净、艾托格列净、度拉糖肽、索马鲁肽、利拉鲁肽、利司那肽、艾塞那肽、阿必鲁肽、口服索马鲁肽;对照组:安慰剂或以上SGLT-2抑制剂、GLP-1受体激动剂中除试验组外的任意一种或多种;④干预时长≥24周;⑤结局指标:主要心血管不良事件、全因死亡、心血管死亡、心力衰竭事件。
-
使用Endnote软件进行文献管理,由2名作者独立阅读文献,按照纳入标准提取研究的一般资料、患者基本特征、结局事件等。如意见不一致,通过讨论或第3名作者介入的方式解决。
-
由2名作者根据Cochrane偏倚风险评估工具2.0独立对纳入研究进行质量评价[15],如意见不一致,通过讨论或第3名作者介入的方式解决。质量评价包括:①随机化过程产生的偏倚;②偏离既定干预措施产生的偏倚;③结局数据缺失产生的偏倚;④结局测量产生的偏倚;⑤结果选择性报告产生的偏倚;⑥整体偏倚。结果表示为“低风险”“需关注”和“高风险”,在5个领域中若出现任意一个或多个偏倚评估为高风险,则整体偏倚评估为高风险。
-
运用R软件 (version 4.0.3) 和GeMTC 包进行贝叶斯网状Meta分析,效应指标为风险比(HR)及其95%可信区间(CI)[16]。运用I2检验来评估研究间的异质性,若I2<50%,表示研究间的误差由抽样误差引起,纳入研究具有同质性;若I2>50%,认为研究间存在异质性[17]。运用节点拆分法检验直接比较结果和间接比较结果是否存在不一致性,若P>0.05,则认为直接比较和间接比较结果一致[18]。运用累积排序概率图下面积(SUCRA)作为累积排序概率的指标,根据SUCRA值的大小对干预措施优劣进行排序,SUCRA值越大表示干预措施获益越多[19]。SUCRA的值介于0到1之间。
-
检索获得18 294篇文献,剔除5 189篇重复文献,通过阅读题目和摘要剔除11 507 篇文献,通过阅读全文剔除1 464篇文献,最后纳入134项随机对照试验(见图1),涉及11种降糖药物。
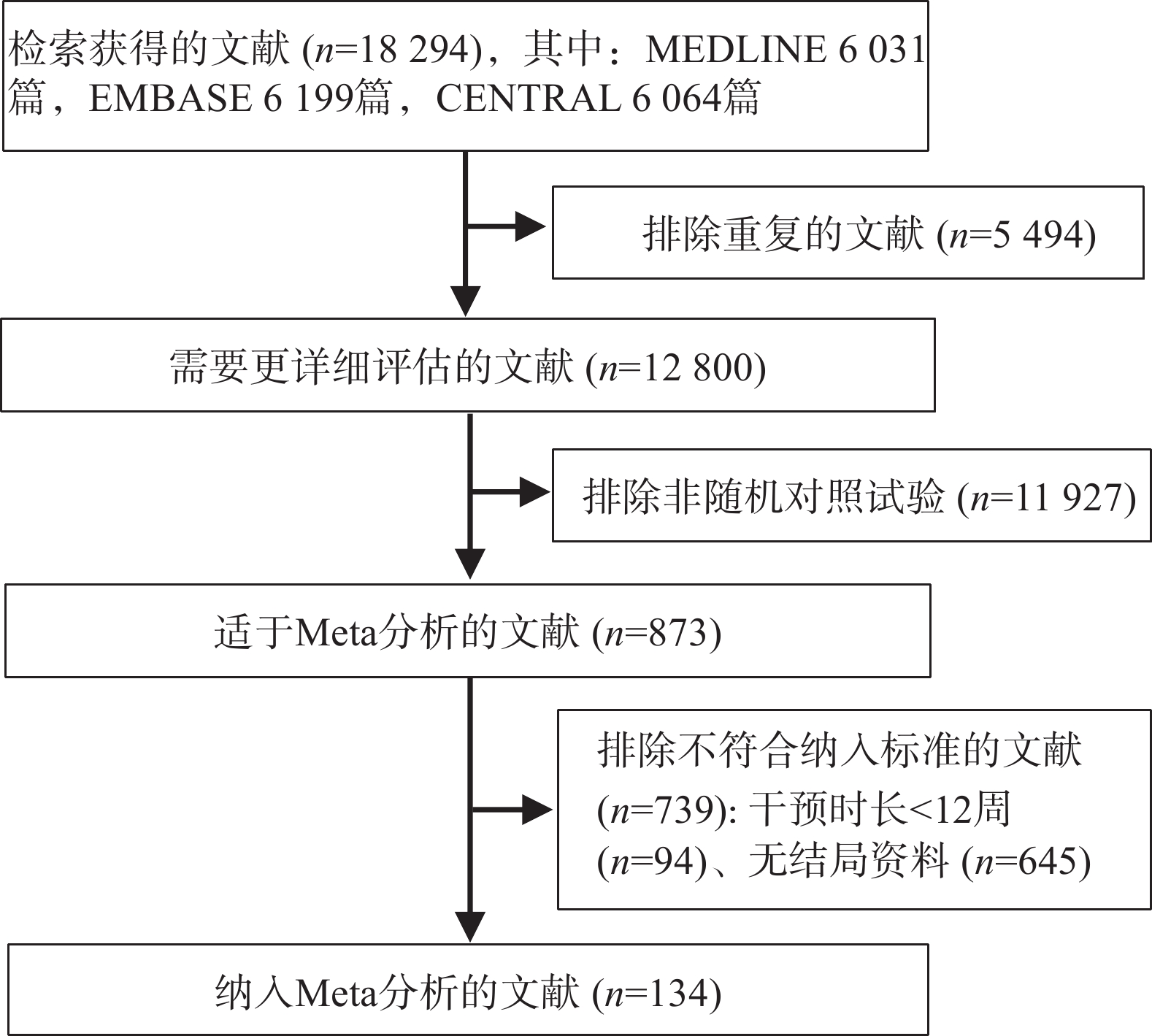
图 1 Meta分析文献纳入和排除流程图
-
共纳入162 345例患者,平均年龄为58.4岁,男性占56.7%,糖尿病病史约9年,平均HbA1c为8.1%,平均空腹血糖为9.2 mmol/L,平均BMI为31.4 kg/m2,平均体重为87.8 kg,平均收缩压为132.2 mmHg,平均舒张压为78.5 mmHg。
-
整体偏倚风险评估中,66项研究为高风险,53项为低风险,14项研究偏倚风险未知。随机化过程、结局测量、结果选择性报告领域中所有研究均为低风险;在结局数据缺失的偏倚评估中,由于研究失访率大于5%、存在组间失访率不均衡,以及缺失的数据等原因,有64项研究为高风险;3项研究因未报告干预分配的分析方法,在偏离既定干预措施的偏倚评估中为高风险。
-
纳入试验的临床特征、方法学及统计学相似,结合异质性检验结果I2=0,表明纳入研究具有同质性。
-
主要心血管不良事件的网状图如图2所示。与安慰剂相比,恩格列净、卡格列净、达格列净、阿必鲁肽、度拉糖肽、艾塞那肽、利拉鲁肽、索马鲁肽,可降低2型糖尿病患者主要心血管不良事件的发生风险(见图3A);与安慰剂相比,恩格列净、卡格列净、达格列净和艾托格列净均可降低2型糖尿病患者心力衰竭的发生风险(见图3B);与安慰剂相比,恩格列净、卡格列净、达格列净、艾塞那肽、利拉鲁肽和口服索马鲁肽可降低全因死亡事件的发生风险(见图3C);与安慰剂相比,恩格列净、卡格列净、利拉鲁肽、口服索马鲁肽可降低心血管死亡事件的发生风险(见图3D)。
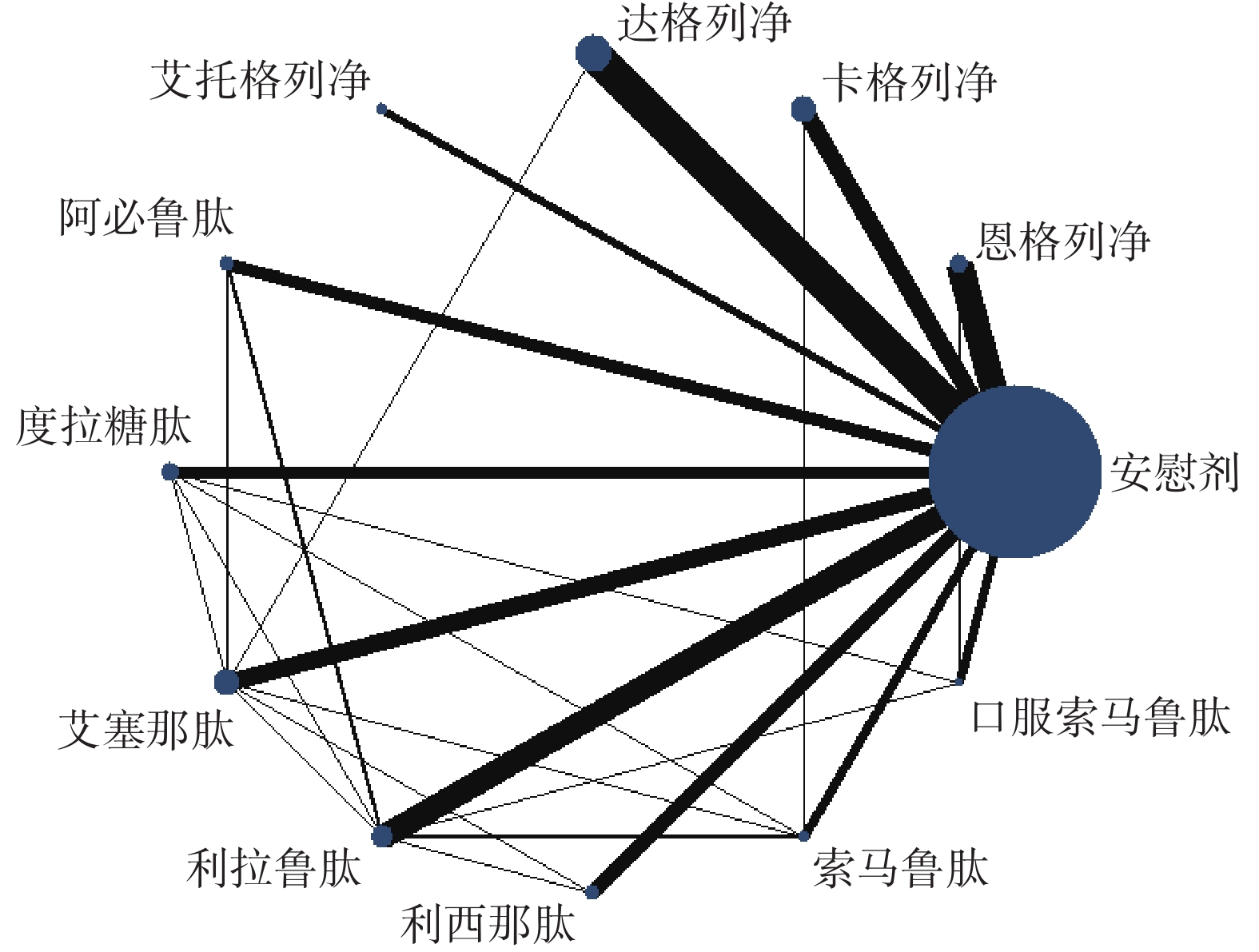
图 2 主要心血管不良事件的网状图
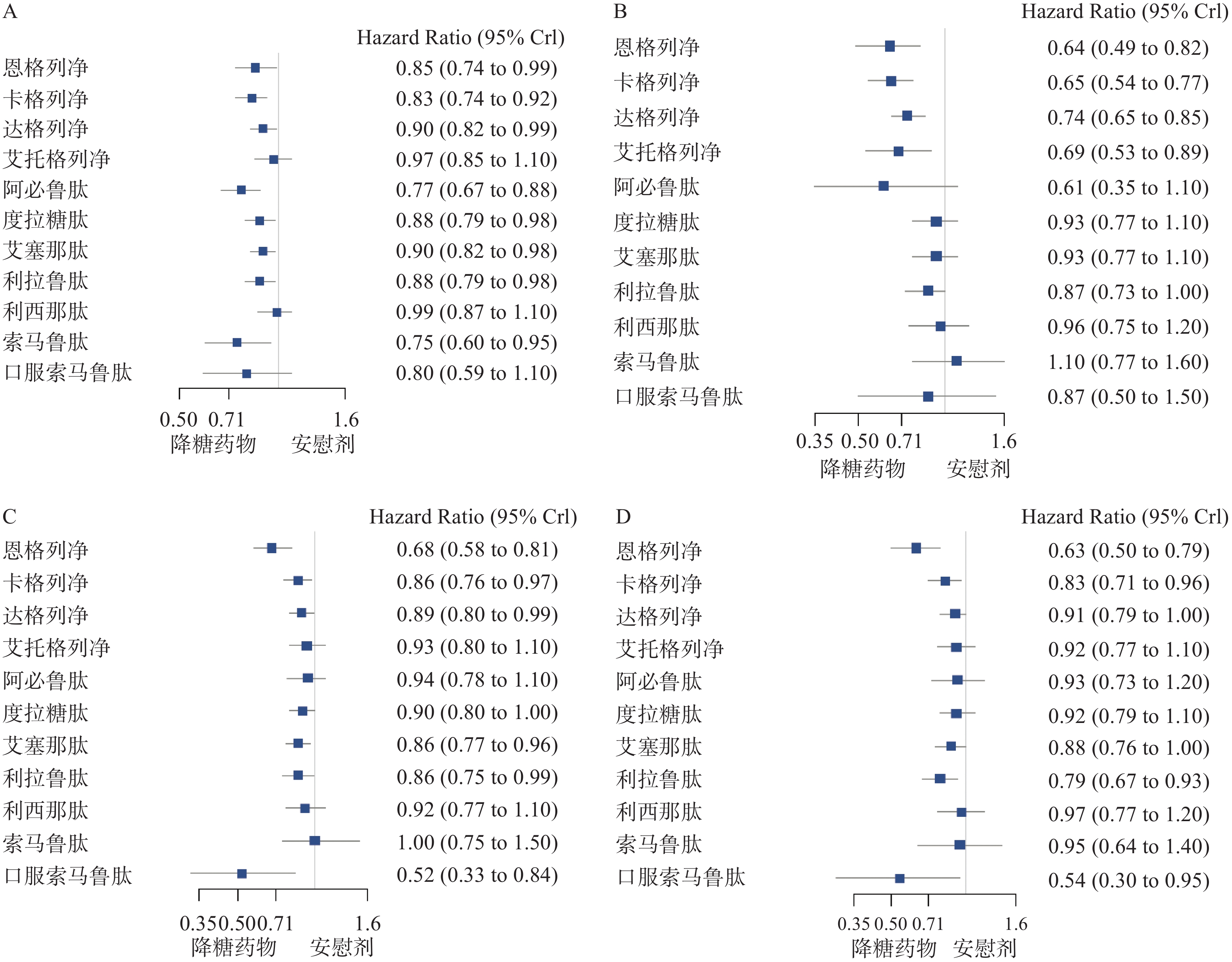
图 3 心血管不良事件终点的森林图
-
纳入研究的网状Meta分析直接证据和间接证据的不一致性检验,P值均大于0.05,表明直接证据和间接证据具有一致性。
-
根据累积排序概率图下面积(见图4),在主要心血管事件方面,获益从高到低的排序依次是:阿必鲁肽、索马鲁肽、卡格列净、口服索马鲁肽、恩格列净、度拉糖肽、利拉鲁肽、艾塞那肽、达格列净、艾托格列净、利司那肽、安慰剂;在降低心力衰竭的发生风险方面,获益排序依次是:恩格列净、卡格列净、阿必鲁肽、艾托格列净、达格列净、口服索马鲁肽、利拉鲁肽、艾塞那肽、度拉糖肽、利司那肽、安慰剂、索马鲁肽。
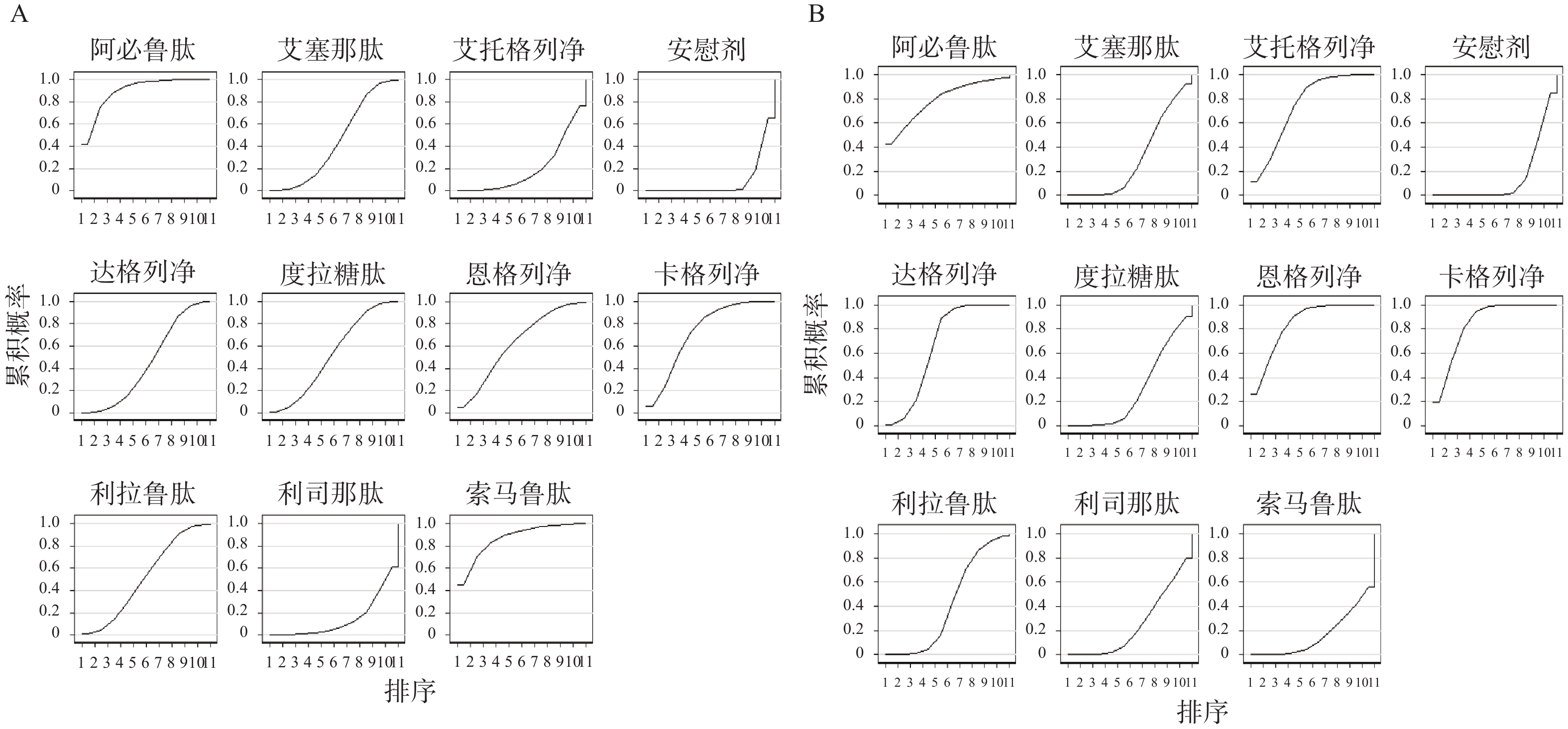
图 4 累积排序概率图及累积排序概率图下面积
-
本文研究结果显示,恩格列净、卡格列净、达格列净、阿必鲁肽、度拉糖肽、艾塞那肽、利拉鲁肽及索马鲁肽可降低2型糖尿病患者主要心血管不良事件的发生风险。结合多项大型心血管安全性试验及最新的循证医学证据,达格列净与艾塞那肽是否具有ASCVD获益还需要进一步研究,目前具有明确ASCVD获益的SGLT-2抑制剂和GLP-1受体激动剂有恩格列净、卡格列净、阿必鲁肽、度拉糖肽、利拉鲁肽和索马鲁肽。在我国可供选择的具有明确ASCVD获益的SGLT-2抑制剂和GLP-1受体激动剂有恩格列净、卡格列净、度拉糖肽、利拉鲁肽。结合本文研究结果,2型糖尿病合并ASCVD患者,应用SGLT-2抑制剂或GLP-1受体激动剂心血管获益从高到低分别是:卡格列净、恩格列净、度拉糖肽、利拉鲁肽。
-
本研究结果显示,恩格列净、卡格列净、达格列净和艾托格列净,均可降低2型糖尿病患者心力衰竭的发生风险,CVOTs及其他循证医学研究与本文研究结果一致,同时4种SGLT-2抑制剂均已进入我国协议期谈判药品目录。结合本文研究结果,降低心力衰竭风险方面,2型糖尿病合并心衰的患者应用SGLT-2抑制剂或GLP-1受体激动剂获益从高到低依次是:恩格列净、卡格列净、艾托格列净和达格列净。
-
前期通过系统检索数据库后发现我国上市的贝那鲁肽、洛塞那肽及tofogliflozin、ipragliflozin等在其他国家上市的SGLT-2抑制剂或GLP-1受体激动剂的随机对照试验较少,报告心血管事件的研究接近于0,因此本研究在制定纳排标准时仅纳入了11种SGLT-2抑制剂和GLP-1受体激动剂。经过筛选后纳入的134篇文献,由于试验失访率高于5%、失访数据存在组间不平衡及失访数据可能影响结果稳定性等原因,在评估偏倚风险时有64项研究在结局数据缺失的偏倚评估中为高风险,为检验研究结果的稳定性,本文通过敏感性分析纳入偏倚风险低的随机对照试验,其结果与主要研究一致。
-
根据本文的研究结果及目前在我国上市的SGLT-2抑制剂或GLP-1受体激动剂,针对2型糖尿病合并ASCVD患者,心血管获益从高到低分别是:卡格列净、恩格列净、度拉糖肽、利拉鲁肽;针对2型糖尿病合并心衰 的患者,应用SGLT-2抑制剂或GLP-1受体激动剂获益从高到低依次是:恩格列净、卡格列净、艾托格列净、达格列净。
Cardiovascular benefits of SGLT-2 inhibitors and GLP-1 receptor agonists in type 2 diabetes: a systematic review and network meta-analysis
-
摘要:
目的 通过贝叶斯网状Meta分析系统评价上市的11种钠-葡萄糖共转运蛋白-2(SGLT-2)抑制剂和胰高血糖素样多肽-1(GLP-1)受体激动剂治疗2型糖尿病患者的心血管获益。 方法 检索Medline、Embase和Cochrane 数据库,检索日期为建库至2020年7月18日。研究终点为心血管不良事件,效应指标为风险比(hazard ratios, HR)及其95%可信区间(95% CI)。 结果 与安慰剂相比,恩格列净、卡格列净、达格列净、阿必鲁肽、度拉糖肽、艾塞那肽、利拉鲁肽和索马鲁肽可降低2型糖尿病患者主要心血管不良事件的发生风险,HR及95%CI为0.75(0.60-0.95) ~0.90(0.82-0.99);恩格列净、卡格列净、达格列净和艾托格列净可降低心力衰竭的发生风险,HR及95%CI为0.64(0.49-0.82) ~0.74(0.65-0.85);恩格列净、卡格列净、达格列净、艾塞那肽、利拉鲁肽和口服索马鲁肽可降低全因死亡的发生风险,HR及95%CI为0.52(0.33-0.84)~0.89(0.80-0.99);恩格列净、卡格列净、利拉鲁肽和口服索马鲁肽可降低心血管死亡事件的发生风险,HR及95%CI为0.54(0.30-0.95) ~0.83(0.71-0.96) 。 结论 应用SGLT-2抑制剂或GLP-1受体激动剂,对2型糖尿病合并动脉粥样硬化性心血管疾病患者的心血管获益依次是:卡格列净、恩格列净、度拉糖肽、利拉鲁肽;对2型糖尿病合并心衰的患者,心血管获益依次是:恩格列净、卡格列净、艾托格列净、达格列净。 -
关键词:
- 钠-葡萄糖共转运蛋白-2抑制剂 /
- 胰高血糖素样多肽-1受体激动剂 /
- 2型糖尿病 /
- 心血管安全性 /
- 网络Meta分析
Abstract:Objective To evaluate cardiovascular benefits in patients with type 2 diabetes mellitus treated with the marketed 11 sodium-glucose co-transporter-2 (SGLT-2) inhibitors and glucagon-like polypeptide-1 (GLP-1) receptor agonism by Bayesian network meta-analysis system. Methods MEDLINE, Embase and Cochrane Library were searched from the establishment of the database to 18 July 2020. The endpoint of the study was adverse cardiovascular events. The effect measures were hazard ratios (HR) and 95% credible intervals (CI). Results Compared with placebo, empagliflozin, canagliflozin, dapagliflozin, albiglutide, dulaglutide, exenatide, liraglutide, semaglutide reduced the risk of major adverse cardiovascular events in patients with type 2 diabetes with HR and 95% CI ranging between 0.75(0.60-0.95)~0.90(0.82-0.99); The risk of heart failure was reduced by empagliflozin, canagliflozin, dapagliflozin and ertugliflozin, with HR and 95%CI ranging between 0.64(0.49-0.82)~0.74(0.65-0.85); Empagliflozin, canagliflozin, dapagliflozin, exenatide, liraglutide and oral semaglutide reduced the incidence of all-cause mortality with HR and 95%CI ranging between 0.52(0.33-0.84)~0.89(0.80-0.99); Empagliflozin, canagliflozin, liraglutide and oral semaglutide can reduce the risk of cardiovascular death events, with HR and 95% CI ranging between 0.54(0.30-0.95)~0.83(0.71-0.96) . Conclusion The order of the cardiovascular benefits of SGLT-2 inhibitors or GLP-1 receptor agonists in patients with type 2 diabetes mellitus complicated with atherosclerotic cardiovascular disease are canagliflozin (the best), empagliflozin, dulaglutide, liraglutide; for patients with type 2 diabetes and heart failure. The order of the cardiovascular benefits for patients with type 2 diabetes and heart failure are empagliflozin, canagliflozin, ertugliflozin, and dapagliflozin. -
药物利用研究(DUR)是促进用药安全、有效和经济的重要手段[1]。随机对照临床试验(RCT)作为评价药物安全性、有效性的金标准,在外推至日常诊疗环境时往往面临挑战。作为RCT的重要补充,真实世界研究(RWS)考察日常诊疗环境中产生的真实世界数据(RWD),注重评价药物使用的“安全性”和“有效性”,已经成为药物利用研究的热点[2]。RWS着眼于应用到医疗实践环境中,大大缩短了试验周期、降低了成本,真实世界实效性临床研究更加易于获取全面的病例数据,使其结果更具有可靠性及可行性[3]。应当正确认识两者关系,将两者作为互补且相辅相成的研究方法和手段来为药物利用评价和监管评价等方面提供循证支持[4-7]。
随着医院管理信息系统(HIS)的高速发展以及高新传感器技术在生物医疗领域探索运用,使得逐步精准化、数字化患者的各项检查及健康诊疗数据成为现实,并进一步完善患者诊疗、实验室检查以及用药信息等全生命周期的医疗记录,且便于追溯及交互关联[2]。尽管数据库技术及大数据挖掘服务于药物安全性、有效性等方面研究成为现实,但应用于DUR尚缺乏具体的技术指导方案、自然流程等。本研究借鉴国内外RWS在药品器械上市后适应证开发及安全性评价方面的做法,梳理DUR中RWS有效技术手段和方法路径,为RWS更好的服务于DUR提供借鉴和参考。
1. 相关概念
DUR是按照预定的标准,评价、分析和解释一个给定的医疗卫生制度下药物利用的模式、质量、影响因素和结果,着重于药物的市场销售、分配、处方和使用情况,强调由此产生的医疗、社会和经济方面的结果。广泛应用于药物流行病学、抗菌药物管理、药物监测、药物警戒等方面的研究。2020年4月,国家药监局发布《真实世界证据支持药物研发与审评的指导原则(试行)》[8],对RWD、真实世界证据(RWE)以及RWS等概念做了相关阐述[8-9]。RWS作为实现从RWD到RWE的有效手段,是连接两者的桥梁[10]。然而,大规模的数据并不一定就能产生有价值的证据,只有通过适用性评估的RWD、分析得出医疗产品的使用和潜在收益或风险的临床证据时才有可能使数据转变为证据[11-12]。数据适用性即从数据使用者角度出发,评价数据满足使用者需求的程度[13],强调数据质量在开展相应RWS方面的可应用程度[14]。
2. 真实世界药物利用研究现状
2.1 真实世界研究与药物利用研究结合现状
国家药品监督管理局自2014年起就陆续出台多项措施,支持RWS用于医疗器械评价、药物审评、研发及监管决策,完善医疗器械不良事件监测和再评价制度,并联合高校、医联体推进多项试点工作的开展,出台了《真实世界研究支持儿童药物研发与审评的技术指导原则(试行)》[15]等法规文件以推进RWS。目前RWS主要集中在以下3个方面:①药物治疗效果[16-17],RWS在药物疗效、不良事件、安全可靠方面的结果研究,以满足药物对人类临床应答的解释以及推广方面应用;②指南或临床实践[18-20],国内外权威的指南是临床实践的重要参考依据,RWS也可用于协助制定和修订患者治疗方案,而RWE有利于指南更加科学性和具有实践性。此外,RWS还可以用于协助政府部门管理的指导性文件的制定;③经济效益[21-23],RWS应用于卫生经济学中筛选研究和治疗选择等方面,帮助医师制定最优的药物治疗方案,并提供合理的经济成本。此外,RWS在帮助制定个性化医疗政策方面也具有很大的潜力。
2.2 真实世界研究体系现状
国际上,随着药品审评和监管标准的不断提高,越来越多的研究者重视RWS,目前已经形成了良好的研究体系,比如美国的以患者为中心的结局研究所(PCORI)和欧盟临床试验公共注册和结果数据库(EUPAS)。RWS主要集中于:①在研究用药的随机对照试验、观察性研究及实践指南中的应用;②在疾病的发病风险评估、医疗健康保险的应用。目前国内的RWS主要涉及:①在中医方面的应用研究[24-26],包括中药的药物疗效及不良反应的研究;②基于医院信息数据库疾病及其合并疾病的用药特征的分析;③在医疗大数据及循证医学方面的应用[27-29]。
RWS的研究设计和方法学也不断完善,近年来不少国家或国际组织都陆续出台关于RWS的指南以及指导原则,提高了RWS的质量和可靠性,比如美国 FDA[30-31]、欧洲EMA[32],英国NICE[33]。
3. 真实世界研究在药物利用研究中的应用
3.1 真实世界药物利用研究的方法
3.1.1 数据来源及研究问题
RWS收集真实诊疗数据或者基于已经存在的研究型数据库或数据研究平台,建立登记数据库,针对具体研究问题,运用循证医学方法,开展数据分析,从而回答验证假设[34-36]。RWD通常来自于以上一个或多个数据库,包含需要主动收集的数据以及常规诊疗行为产生的临床数据。随着医学大数据的快速发展,一些研究型数据库或数据研究平台也逐步拓展,目前,国内外利用公共数据库如SEER、MIMIC等进行相关研究已成为RWS的重要发展方向。
RWS通常基于研究目的建立研究数据库或数据集,研究要素一般包含目标患者人口学特征、用药信息、门诊、住院信息、实验室检查、治疗转归与结局,以及其他研究目的所涉及到的临床治疗、护理、手术处置等信息。如果数据来自多个不同数据库,还必须通过如患者身份证号码、住院号/检查号、姓名等患者唯一标识码进行辨识和数据关联。如果研究的资料内容涉及到患者的个人信息等情况,还要注意取得伦理学审核以及保护患者隐私[37-41]。真实世界DUR的药品数据通常通过ATC编码来规范,采用用药依从性,限定日剂量(DDD)、平均治疗天数(ATD)、总DDD数、处方年费用等DUR指标[42]。基于药物效果和安全性研究、经济学和药物政策、多个疾病和多个治疗方案的复杂病情分析是当前真实世界药物利用研究的一个热点。
RWS作为一项非随机、开放性、不使用安慰剂的研究。为了挖掘真实的临床医疗环境产生的诊疗数据,应把质量控制作为全局指标来进行把握,并从研究伊始就建立起全面的数据质量控制方案并严格遵守。同时,在研究中详细记录异常情况[43],还要注意数据清洗以及混杂因素的控制,如此才能保证研究证据的质量及等级[44]。
3.1.2 研究人群及纳排标准
RWS人群纳入条件较为宽松,但仍在研究中需要明确与研究目的相关或可能影响研究的因素,以及纳入及排除标准的研究时间段和制定日期。研究通常通过WHO国际疾病分类(ICD-9/10)筛选研究人群。研究人群通常为患有特定疾病的患者、药物使用者(罕见病、孕妇、儿童等)以及患有多种疾病的复杂病例或有多种伴随症状的人群。有时候为解决研究对象以往接受过某种治疗措施可能导致的选择偏倚,还需要考虑遵照首次用药人群的设计[45]。最后,研究者需谨慎纳入和排除标准,以免直接影响研究结果的外推。
研究者应当严格参照PICOTS原则明确的6个关键点(总体、干预、比较对象、结果、时间和场所),同利益相关者一同提出针对研究问题可利用的科学方法[46]。
3.1.3 真实世界药物利用研究设计
观察性研究设计是RWS中广泛使用的设计类型之一[44],常见的有前瞻性观察研究[47]、回顾性队列研究[18,48]、Meta分析[49]等。根据不同的研究目的和研究对象,可以选择适合的研究方法和样本来源,通常需要开展大规模、跨学科的合作,以确保研究结果的可靠性和科学性。RWS设计时要结合研究目的来具体确定研究要素,综合考虑年龄、混杂偏倚和特殊人群、药品ATC编码,以及病历等非结构化数据。设计通常包括以下几个阶段:①定义问题:在研究开始之前明确研究的目的和问题,确定研究的对象、变量和数据采集方式。需要考虑研究的可行性、科学性和意义。②研究设计:根据定义的问题,制定设计方案。明确设计类型、样本容量、数据采集方式、结局指标以及数据分析方法等。③招募研究对象:确定研究对象的选择标准,并依照这些标准进行样本招募。④数据收集和管理:采集所需的研究数据,将收集到的数据进行规范化、清洗、质量控制和审查等处理。⑤数据分析:使用统计学方法进行数据分析,包括描述性统计、回归分析、生存分析和成本效益分析等。⑥结果解释和推广:将研究结果进行整合、解释和推广,发表研究报告和文章,向目标受众,如医师、政策制定者、患者和公众等,传达研究结论和建议。
3.1.4 特征变量及评价指标
RWS设计阶段应该充分了解现有数据的优缺点,并恰当合理的定义并描述暴露因素,尽可能的收集与暴露相关的特征指标。RWS结局指标是评估一种治疗或干预措施在真实医疗实践中的效果和安全性以及相关临床和经济结果的指标。
通常有以下几种结局指标:①主要疗效结局:主要的成果、结果或效果指标。例如,治疗效果、复发率、临床终点事件;②次要疗效结局:主要疗效结局之外的其他疗效结果或事件。如总体存活率(OS)、无进展生存期(PFS)、无病生存期(DFS)、疾病进展时间(TTP)、治疗失败时间(TTF)、死亡率,住院时间等[50];③安全性结局[12,51]:一般采用药物不良反应(ADR)、不良反应发生率(IRs,通常以1000人/年表示)[12]、危险性信号、药物相互作用等;④经济学结局[52-53]:包括成本效益和成本效用评估、日均费用、医疗保险、社会资源利用及患者的自付费用等。
选取结局指标时需要根据研究目的和研究对象,进行目标导向和可行性评估。常规首选应该是临床意义明确和易于全面评估的主要疗效结局,同时可以考虑次要疗效结局和安全性结局作为辅助评估。为综合评估治疗效果和成本并获得系统的经济评估结果,相关经济学方面的评价指标也应该考虑进来。
3.2 统计及敏感性分析
通常对目标患者群体和治疗模式进行描述性统计分析,分析各分类变量的频率、百分比,以及在连续区间尺度上测量的变量平均值、标准差、中位数及范围,有学者应用Kaplan-Meier(KM)生存函数进行相关生存分析[54]。针对研究目标确定分析要素,选用合适的统计分析方法,如卡方检验、logistic回归和多元线性回归等,对治疗结局、暴露因素、协变量数据类型及分布情况进行校正分析。由于所有研究结果基于假设提出,而这些假设往往是推论真实性的依据。研究者需对数据的局限性和问题本质有清晰认识,研究过程中对假设进行调整,评价观察结果对特定假设的敏感度或方向大小上的一致性。
3.3 混杂因素及偏倚控制
3.3.1 混杂因素
RWD来源包含电子病历、医保数据库、生命体征记录、医学图像等,存在许多复杂的混杂因素。混杂因素可能的类型包括个体基线特征、随时间变化的特征、医疗诊断和治疗、环境因素。常见的混杂控制策略包括随机对照、匹配分析、协变量校正、倾向值和剂量反应模型等。除此之外,在实施RWS时,还要注意有代表性的样本选择,对数据质量和分析偏倚进行评估和控制,以获得准确和可靠的研究结论。
3.3.2 偏倚控制
RWS是在真实临床环境下进行的研究,目标人群的治疗措施因非随机分配影响内部真实性,虚弱个体治疗措施与结局之间的关联性等,使得其研究结果可能存在一定的偏倚,这些偏倚可能影响研究的可靠性和有效性。常见的偏倚类型包括选择性偏倚、信息偏倚[55]、报告偏倚、记忆偏倚等,常见的偏倚控制方法有模拟试验、设计分层、倾向值匹配、重复量表、级联分析等。
4. 展望
真实世界DUR作为一种新兴的药物评价方法,可将从真实世界环境下收集和分析的大量数据利用起来,通过实效性、回顾性研究使得过往产生的既有诊疗数据进一步提炼成RWE而二次利用。通过研究分析获得的循证医学证据,可以为DUR提供有价值的依据,帮助优化药物使用、个体化医疗、提高患者结局、降低医疗费用、促进医学的健康发展;也可采用前瞻性研究大样本或特殊人群,为其更好、更安全有效用药提供证据。
同时,RWS也是评价药物滥用的有效手段。随着大数据和医疗技术的不断发展,RWS将会成为药物治疗效果、患者治疗策略和临床实践方面重要的研究领域,并将不断地推动医药的创新、优化和进步。
值得注意的是,RWS是一项复杂的研究工作,需要具备较强的统计、数据挖掘和医学知识背景,同时也面临着数据质量、缺失值、样本匹配和结果影响因素多等问题。因此,在实施RWS时,需要有效的科学设计、广泛报告,同时进行敏感度分析和可能存在的偏差分析,为制定更加科学和有效的药物治疗方案提供科学支持。
-
图 2 主要心血管不良事件的网状图
注:图中的圆形代表一种治疗措施,圆形大小与接受该治疗措施的患者人数呈正比;连线代表两种治疗措施之间有直接比较,连线的粗细与研究数量呈正比
图 3 心血管不良事件终点的森林图
注:A.主要心血管不良事件(128项研究, 161 460例患者);B. 心力衰竭事件(66项研究,130 646例患者);C. 全因死亡事件(78项研究,140 487例患者);D. 心血管死亡事件(66项研究,130 646例患者)
-
[1] ZINMAN B, WANNER C, LACHIN J M, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes[J]. N Engl J Med,2015,373(22):2117-2128. doi: 10.1056/NEJMoa1504720 [2] NEAL B, PERKOVIC V, MAHAFFEY K W, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes[J]. N Engl J Med,2017,377(7):644-657. doi: 10.1056/NEJMoa1611925 [3] WIVIOTT S D, RAZ I, BONACA M P, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes[J]. N Engl J Med,2019,380(4):347-357. doi: 10.1056/NEJMoa1812389 [4] CANNON C P, PRATLEY R, DAGOGO-JACK S, et al. Cardiovascular outcomes with ertugliflozin in type 2 diabetes[J]. N Engl J Med,2020,383(15):1425-1435. doi: 10.1056/NEJMoa2004967 [5] PERKOVIC V, JARDINE M J, NEAL B, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy[J]. N Engl J Med,2019,380(24):2295-2306. doi: 10.1056/NEJMoa1811744 [6] MARSO S P, DANIELS G H, BROWN-FRANDSEN K, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes[J]. N Engl J Med,2016,375(4):311-322. doi: 10.1056/NEJMoa1603827 [7] MARSO S P, BAIN S C, CONSOLI A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes[J]. N Engl J Med,2016,375(19):1834-1844. doi: 10.1056/NEJMoa1607141 [8] HOLMAN R R, BETHEL M A, MENTZ R J, et al. Effects of once-weekly exenatide on cardiovascular outcomes in type 2 diabetes[J]. N Engl J Med,2017,377(13):1228-1239. doi: 10.1056/NEJMoa1612917 [9] PFEFFER M A, CLAGGETT B, DIAZ R, et al. Lixisenatide in patients with type 2 diabetes and acute coronary syndrome[J]. N Engl J Med,2015,373(23):2247-2257. doi: 10.1056/NEJMoa1509225 [10] HERNANDEZ A F, GREEN J B, JANMOHAMED S, et al. Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes): a double-blind, randomised placebo-controlled trial[J]. Lancet,2018,392(10157):1519-1529. doi: 10.1016/S0140-6736(18)32261-X [11] GERSTEIN H C, COLHOUN H M, DAGENAIS G R, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial[J]. Lancet,2019,394(10193):121-130. doi: 10.1016/S0140-6736(19)31149-3 [12] HUSAIN M, BIRKENFELD A L, DONSMARK M, et al. Oral semaglutide and cardiovascular outcomes in patients with type 2 diabetes[J]. N Engl J Med,2019,381(9):841-851. doi: 10.1056/NEJMoa1901118 [13] 中华医学会糖尿病学分会. 中国2型糖尿病防治指南(2020年版)[J]. 中华内分泌代谢杂志, 2021, 37(4):311-398. doi: 10.3760/cma.j.cn311282-20210304-00142 [14] 赖彦岚, 黄爱文, 张丽丽, 等. SGLT-2抑制剂和GLP-1受体激动剂的心血管安全性研究进展[J]. 药学实践杂志, 2020, 38(6):496-500,567. doi: 10.12206/j.issn.1006-0111.202006061 [15] 杨智荣, 孙凤, 詹思延. 偏倚风险评估系列: (二)平行设计随机对照试验偏倚评估工具2. O介绍[J]. 中华流行病学杂志, 2017, 38(9):1285-1291. doi: 10.3760/cma.j.issn.0254-6450.2017.09.028 [16] SPIEGELHALTER D J, BEST N G, CARLIN B P, et al. Bayesian measures of model complexity and fit[J]. J Royal Stat Soc Ser B Stat Methodol,2002,64(4):583-639. doi: 10.1111/1467-9868.00353 [17] VERONIKI A A, VASILIADIS H S, HIGGINS J P T, et al. Evaluation of inconsistency in networks of interventions[J]. Int J Epidemiol,2013,42(1):332-345. doi: 10.1093/ije/dys222 [18] SALANTI G, ADES A E, IOANNIDIS J P A. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: an overview and tutorial[J]. J Clin Epidemiol,2011,64(2):163-171. doi: 10.1016/j.jclinepi.2010.03.016 [19] CHAIMANI A, HIGGINS J P, MAVRIDIS D, et al. Graphical tools for network meta-analysis in STATA[J]. PLoS One,2013,8(10):e76654. doi: 10.1371/journal.pone.0076654 期刊类型引用(0)
其他类型引用(1)
-

 点击查看大图
点击查看大图
计量
- 文章访问数: 5189
- HTML全文浏览量: 1981
- PDF下载量: 26
- 被引次数: 1
